


Healing our Hearing
Breakthroughs in protecting kids' cochleas from chemotoxicity

I wrote before about the sense of smell, but this is the first newsletter discussing breakthroughs in understanding inner ear physiology and pharmacology. Many times, parents and pediatricians are faced with the Sophie’s Choice between treating life threatening cancer or sepsis with a critical drug that would likely cause deafness as its tradeoff. Tough decisions. But now we seem to have several options that can lessen the risk of that nasty outcome.

To hear, incoming sound waves hit the tympanic membrane, get transduced by the middle ear bones to produce fluid waves inside the cochlea, causing the basilar membrane to flex, thus bending the stereocilia attached to the tectorial membrane. This mechanocompression induces action potentials in the hair cells (HC). They then release an excitatory neurotransmitter at a synapse with a sensory neuron, which conducts action potentials to the central nervous system via the cochlear branch of the vestibulocochlear cranial nerve.
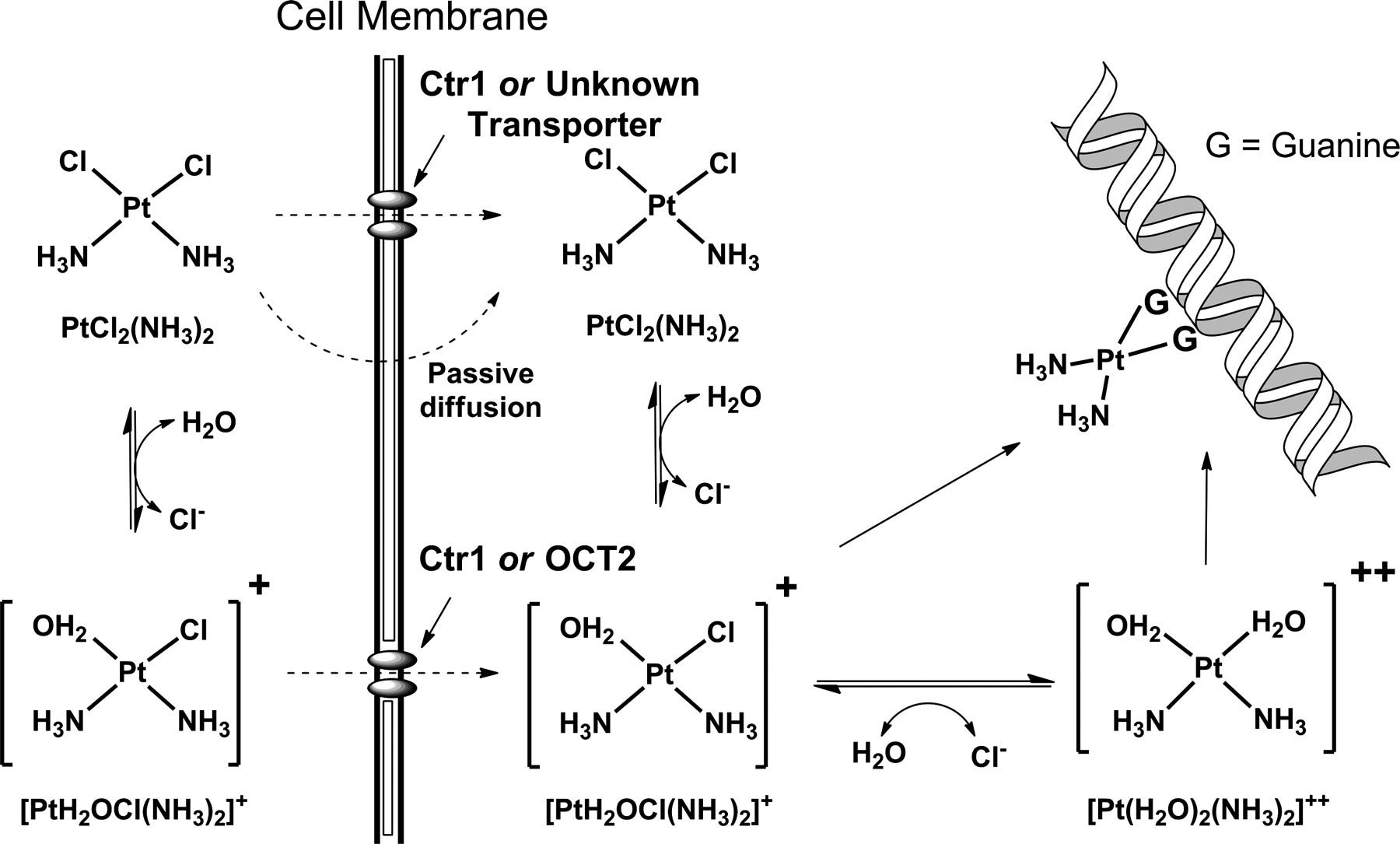
Recently we learned about membrane drug transporters and eventually researchers got around to investigating their roles in the cochlea. There, they explored the influx and efflux kinetics of the copper transporter (CTR) and organic cation transporter (OCT). Soon they discovered that the chemotherapy drug cisplatin utilizes those pathways to enter tumor cells; unfortunately it also enters the hair cells lining the basilar membrane, causing their death.

Rescuers of Cisplatin Ototoxicity
Over the last decade, several researchers explored ways to prevent hearing loss from exposure to toxins. In particular, the utility of cisplatin was severely limited because of its ototoxic effects.
Studies of cisplatin-induced ototoxicity and cochlear uptake show that it can be modulated by administration of a CTR1 inhibitor, copper sulfate. In mice, intratympanic administration of copper sulfate given before intraperitoneal cisplatin dosing prevented subsequent hearing loss.
In organotypic tissue culture preparations, another lab found that pretreatment with the drug transporter inhibitor, cimetidine, could prevent the loss of hair cells after cisplatin exposure.
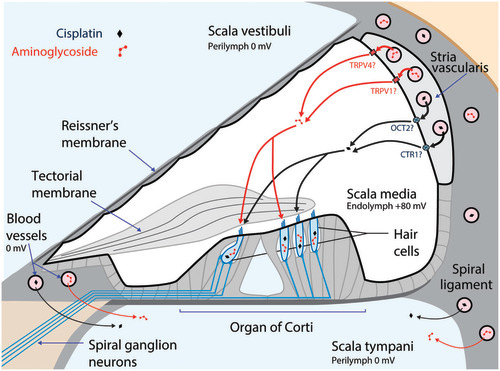
In studies with guinea pigs, cisplatin induced electrophysiological threshold shifts, hair cell loss, and reduced synaptophysin immunoreactivity in the synapse area around the inner HCs and outer HCs. Cisplatin also reduced the OCT2 intensity in the inner and outer pillar cells and in the stria vascularis as well as the CTR1 intensity in the synapse area around the inner HCs, the Deiters’ cells, and the stria vascularis. Hydrogen gas inhalation treatment given for 60 min starting immediately after guinea pigs received a single cisplatin injection mitigated all these effects. Gaseous H2 is safe at levels <4% of atmospheric air, and does not induce adverse reactions in humans. The proposed mechanism of action of its otoprotection may be via changes in redox potential, but clearly it is correlated somehow with the density of the transporters.
Drugs containing thiol groups have a high affinity for cisplatin. So there is the possibility they could interfere with the therapeutic effects of cisplatin. But sodium thiosulfate was safely administered systemically, with minimal antitumor interference, when given 4 to 6 hours after cisplatin dosing.
Actual clinical trials with children undergoing chemotherapy did test the compound, sodium thiosulfate (STS). It was administered six hours after cisplatin dosing to see whether it would reduce the severity of hearing loss without affecting the chance of cancer cure. The clinical trial involved 116 children with primary liver cancer, hepatoblastoma. Of the participants who did not receive STS, 66 % suffered hearing loss, compared with only 33 % of those who received STS. Importantly, STS treatment exhibited no apparent interference with antitumor efficacy.
Sodium thiosulfate’s actions on the copper and organic anion membrane transporters is unknown. Like hydrogen gas, it may interact with the redox potential at the membrane transport site. The reaction between copper ions and thiosulfate is likely a combination of redox electrochemistry and coordination chemistry. Compounds formed in their reactions will depend on the concentration of the reactants and their relative total amounts in the environs. So, like the recent newsletter about RBC membrane electrochemical potentials, perhaps the external electrochemical gradient may play a role.
But the bottom line message for kids with cancer is … we now have some treatments that do work! Let the hearing healing begin.
REFERENCES
CJ Kros, PS Steyger. Aminoglycoside- and Cisplatin-Induced Ototoxicity: Mechanisms and Otoprotective Strategies. Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a033548 http://perspectivesinmedicine.cshlp.org/content/early/2018/12/17/cshperspect.a033548.full.pdf
PS Steyger Mechanisms of Aminoglycoside- and Cisplatin-Induced Ototoxicity American Journal of Audiology Review Article 11 Oct 2021 https://pubs.asha.org/doi/10.1044/2021_AJA-21-00006
SS More et al. Role of the Copper Transporter, CTR1, in Platinum-Induced Ototoxicity. The Journal of Neuroscience, July 14, 2010 • 30(28):9500 –9509
HE Jing-chun et al. Modulation of copper transporters in protection against cisplatin-induced cochlear hair cell damage. Journal of Otology 2011 Vol.6 No.2
PR Brock et al. Sodium Thiosulfate for Protection from Cisplatin-Induced Hearing Loss, New England Journal of Medicine (2018). DOI: 10.1056/NEJMoa1801109
AE Fransson et al (2017) Hydrogen Inhalation Protects against Ototoxicity Induced by Intravenous Cisplatin in the Guinea Pig. Front Cell Neurosci 11:280 doi: 10.3389/fncel.2017.00280
MP Hughes et al. Vm‐related extracellular potentials observed in red blood cells. https://www.nature.com/articles/s41598-021-98102-9